
Dosimeter badge services for medical, dental, and veterinary businesses
Learn how Radiation Detection Company’s easy-to-use dosimetry solutions can boost the efficiency of your practice.
Written by
Chuck Nagel
Healthcare Business Partner
Last Updated: December 20, 2025
As DBT, CEM, and advanced breast imaging technologies become standard in mammography, radiation safety programs must evolve with them. This article explains how modern modalities influence scatter conditions, workflow proximity, dose trends, and what imaging leaders should prioritize to protect staff and strengthen compliance.
In my years overseeing imaging departments, one thing became increasingly clear: technology changes faster than many safety programs can keep up. Mammography is no exception. Digital breast tomosynthesis (DBT) has become the standard in many facilities. At the same time, contrast-enhanced mammography (CEM) is expanding rapidly as a lower-cost, highly accessible alternative to MRI. Even biopsy systems now rely on multi-step imaging workflows that look very different from traditional 2D mammography.
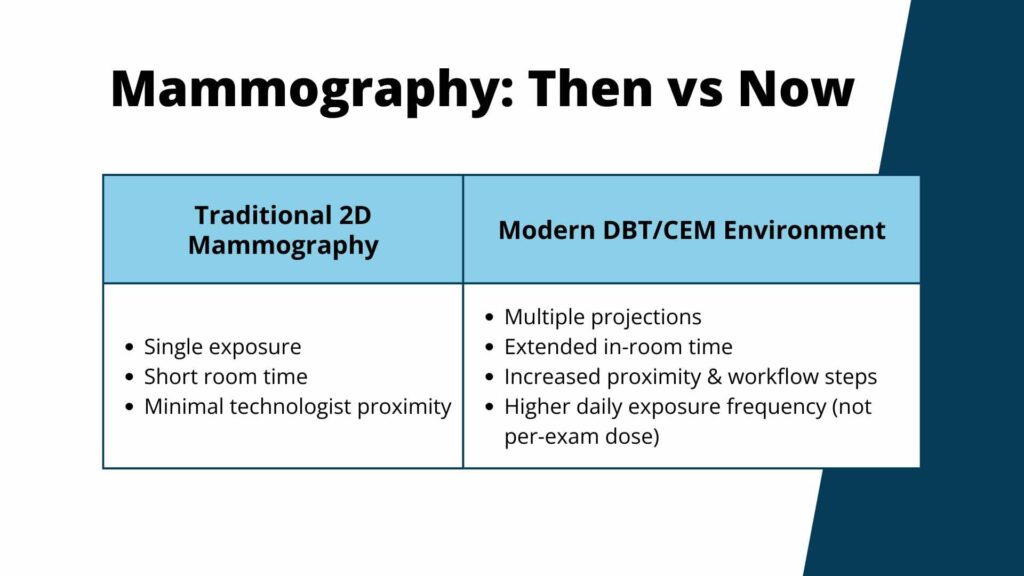
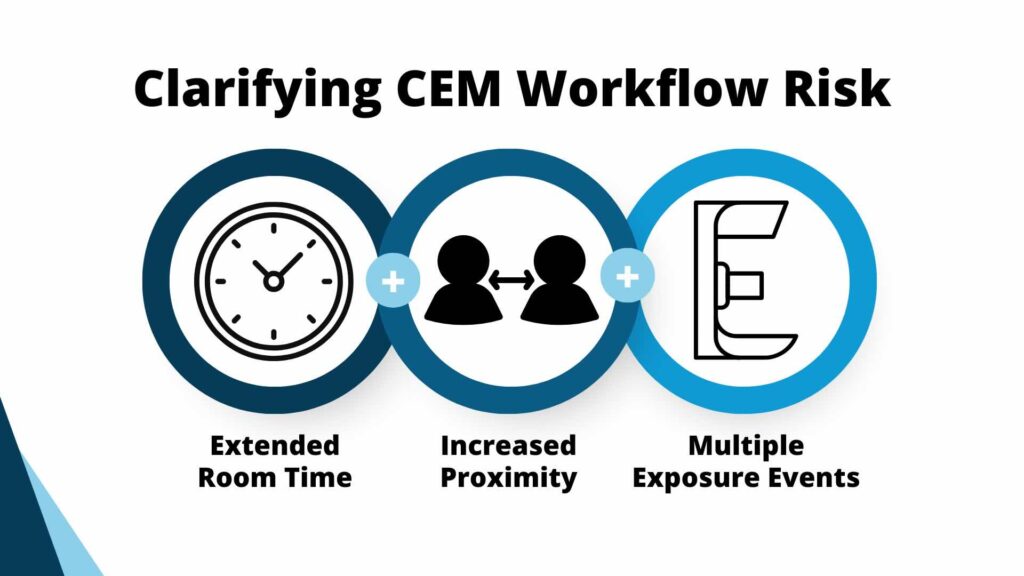
These technologies deliver enormous clinical value, but they also reshape the exposure landscape in ways that hospital imaging directors, RSOs, physicists, and technologists must account for. Modern modalities alter scatter patterns, increase throughput, extend room time, and create more exposure opportunities throughout the day.
While the 2024 MQSA update focused on reporting, breast density communication, and outcomes audits (and not radiation dose explicitly) it also reinforced an important truth: Accrediting bodies expect consistent performance backed by traceable, data-driven documentation. Radiation safety is now part of that ecosystem.
To protect staff and remain inspection-ready, mammography programs must evolve beyond legacy assumptions and adapt to how imaging is actually performed in the real world.
DBT acquisitions involve multiple projection images and a sweeping X-ray tube motion. Although each exposure is low, the frequency of exposures per technologist has increased significantly.
From my experience managing DBT adoption, technologists spend more time at the gantry during positioning and repeat adjustments, leading to higher throughput and more total exposure events per shift.
Scatter behaves differently compared to traditional 2D mammography. For radiation safety programs, this means dose trend reviews should now be evaluated against DBT volume, not just badge cycles.
DBT exposure is less about one exam and more about the cumulative effect of workflow patterns throughout the day.
Dosimetry violations are becoming a top enforcement priority for regulatory bodies. Learn why regulators are cracking down on dosimetry violations (and how to stay compliant).
While CEM is a major step forward in diagnostic mammography, imaging departments need to be aware of the radiation safety considerations.
For example, dual-energy acquisitions increase the total dose per exam. Technologists will need to spend longer periods in-room due to contrast workflows, and repeated views may be necessary depending on enhancement patterns.
In the hospital environments I’ve worked in, our early CEM adopters saw exposure variances that only became clear once we reviewed real badge data. The modality itself wasn’t the issue – the workflow demand, however, was.
Effective radiation safety programs must now account for CEM-specific training, ALARA review, dose trend monitoring, room configuration, and proximity analysis. These considerations further highlight the importance of personnel and area dosimetry.
Modern mammography-guided biopsy systems reduce patient discomfort and improve targeting, but they still require multiple scout images, repositioning steps, and scatter conditions that differ from standard screening rooms.
These environments benefit from a combination of area monitoring (to validate real scatter conditions), and personnel monitoring for technologists supporting biopsy workflows.
Biopsy suites should not be treated as static, low-dose environments. Their workflow-driven exposure patterns make them critical elements of a comprehensive safety program.

The MQSA Final Rule that went into effect in September 2024 strengthened requirements around reporting and documentation clarity, breast density notification, outcomes auditing, and traceability.
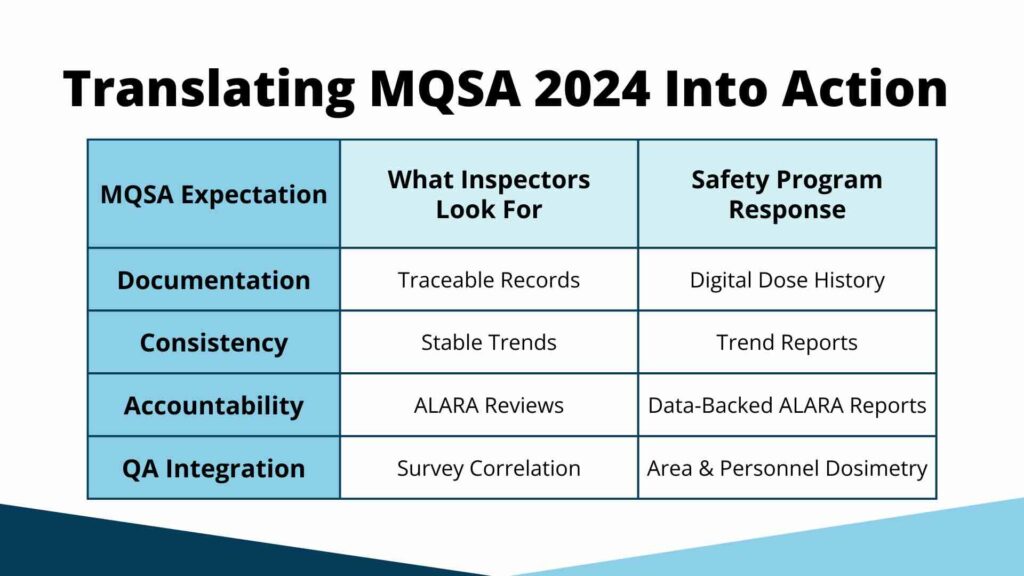
While it did not introduce new radiation protection limits, MQSA’s emphasis on consistency and verifiable documentation raises expectations for how facilities demonstrate safety, including
In short, radiation safety is now expected to reflect the same level of performance accountability as reporting and quality metrics.
Here’s what you need to know about the new standard for radiation safety performance – and what you can do to get ahead.
Inspectors increasingly ask how dose trends have changed with DBT and CEM adoption. Staff exposure should remain stable, even as modality volumes rise.
Facilities that can show this with clear, digital data will be ahead of the curve and stand out in terms of audit readiness.
At Radiation Detection Company, we offer centralized, exception-based reporting through MyRadCare Insights™ – a powerful radiation safety analytics platform designed for healthcare systems that demand better visibility, faster decision-making, and lower compliance risk.
Modern modalities create more variables for physicist testing and shielding verification. Digital dosimetry helps teams correlate real-world scatter conditions and equipment performance over time.
This proactive approach automatically accounts for workflow-related exposure changes, creating a unified safety and QA ecosystem.
Outdated ALARA approaches based solely on 2D mammography no longer meet operational reality.
Modern ALARA reviews should include:
This change should shift how imaging departments approach ALARA – taking it from a reactive process to a proactive safety tool.
Looking for guidance on radiation safety and compliance? Our compliance experts built a Radiation Compliance Cheat Sheet to help you quickly identify and address gaps that can put your organization and employees at risk.
Annual physicist surveys provide a controlled snapshot. Area dosimetry helps fill in any gaps outside of the survey window to proactively alert departments to any changes that could put patients and staff at risk.
Together, they create a complete picture of operational exposure conditions.
Radiation compliance standards vary widely from state to state. Our comprehensive 50 State Guide to Radiation Safety helps you navigate compliance guidelines and keep your team safe.
Radiation Detection Company (RDC) has provided true operational value for over 40,000 organizations since 1949. RDC is the ideal dosimetry provider for mammography departments because they offer:
Radiation Detection Company has the technical expertise and proven reliability to help imaging leaders modernize their radiation safety programs with data they can trust.
To strengthen your mammography radiation safety program, call RDC at 800.250.3314 or reach us through our contact page.
Not inherently, but higher workflow frequency and prolonged positioning can increase exposure opportunities. Monitoring trends is essential.
Dual-energy imaging and extended in-room time can increase cumulative exposure. Dose tracking should reflect CEM workflow factors.
No. But its emphasis on documentation and consistency raises expectations for transparent exposure history and ALARA performance.
They should evaluate modality-driven trends, room-specific scatter conditions, technologist roles, and corrective actions tied to measurable dose data.
Digital dosimetry enables exposure trend analysis, QA integration, quick documentation retrieval, and stronger inspection readiness.
Learn how Radiation Detection Company’s easy-to-use dosimetry solutions can boost the efficiency of your practice.



